If you physically acquire 10–1,000 active particles of coronavirus, low viral load, your chances of catching Covid-19 are almost zero. In fact you can probably pick up more than that as a lot of the viral particles will be inactive so effectively harmless.
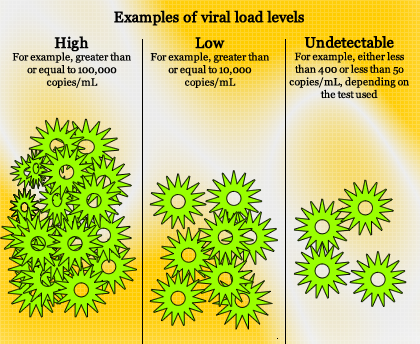
Now if you somehow come into contact with an infected droplet that might have about 1 billion active particles of coronavirus and subsequently transferred 100 million active viral particles to your face scratching your nose or wiping your eye then the chances are you have a very good chance of catching the disease.
What we are talking about is viral load and the possibility of active particles being around to infect people and perpetuate the disease is greater if the environment is cold, wet and dark than if the weather is hot dry and sunny. Sunshine has ultraviolet rays that damage the RNA that makes up the virus.
Viral load has a big part to play in the severity of the disease as well.
There is evidence that the infectious dose received at the time of infection dictates the severity of the disease and repeated infection doses leads to more severe cases. Health care workers might receive an infectious dose and whist that initial infection is multiplying in one area of the body then receive a second or third dose before symptoms become apparent.
At the moment we do not know exactly how many viral particles are needed to make up an infectious dose. That is the number of particles needed to effectively multiply in your body and overwhelm your defences. It is reasonable to assume that that viral load might be a minimum of at least 10,000–100,000 viral particles. It is also likely that genetics might play a part in susceptibility coupled with the strength of the person’s immune system. Their immune history will clearly be relevant so whether they had seen a similar coronavirus before (SARS or MERS for example). It is also possible that some people are naturally immune.
All this assumes that the virus is transmitted through droplets containing the virus, however, we also suspect that at least some transmission of the disease might occur through airborne transmission it seems likely though that the infectious dose from airborne transmission would be unlikely to have the numbers of particles needed to cause a severe case of the disease.
What is significant though is that the exposure of the virus at low or negligible viral load through the two mechanisms mentioned above would deliver enough SARS Cov-2 virus to trigger the initial production of T-cells in the blood of uninfected patients. It would not be enough to cause the production of antibodies as the individual has not received an infectious dose.
The explanation given for the DOCC theory (Decline of Covid-19 cases) had identified but not explained the phenomenon of uninfected individuals having Covid-19 specific (Sars Cov-2) T-cells. An understanding of how we can be exposed to low levels, (low viral load) of virus without being infected might now be apparent. Wheras before people have avoided at all costs getting physically close to the virus. It now seems that weak exposure may actually be beneficial as long as there is not repeated exposure. What would seem critical is the length of time needed for the body to build up a level of T-cells capable of fighting of a more significant attack.
Our immune status assumes that the person starts from zero immunity of course. In fact many of us may well have a residual supply of T-cell from previous coronavirus encounters. The problem remains however, that with a now recognised high proportion of asymptomatic individuals we have no way of assessing our level of exposure, so inevitably it’s back to hand washing and social distancing to be as safe as possible.